Capitalizing on the Continuum: Module 2 – The Continuum of Care
June 15, 2022 by Steve Kerschke, PT
From the ICU through community-based care, the Continuum of Care covers each stage of the recovery journey. In this module, Steve Kerschke, PT and Brad Dexter, DPT of Kintinu Telerehab discuss the levels of the Continuum of Care and explain how each one relates to time, outcome predictability, and levels of care.
Speakers: Steve Kerschke, PT and Brad Dexter, DPT
Video Transcription
Introduction
Brad Dexter PT, DPT [00:08]:
This is Part 2 going through a series regarding capitalizing on the continuum. So, just knowing that there are lots of different levels of care. This module is devoted to understanding that continuum of care within rehab.
Steve Kerschke, PT [00:23]:
Remembering, we’re also talking about catastrophic injury. Anytime we’re talking about the continuum, many of these individuals, for sure, are going to hit the first parts. Then we get down to the second couple, and those become a bit more situational.
What Are the Levels of the Continuum of Care?
So today we’ll start with talking about what are the levels of the continuum. Brad now will go through a little bit of detail for each one. Then we’ll expand a little bit more on some of the keys along the way, some of the aspects that can lead to trouble or, if navigated well, hopefully it leads to a really great outcome.
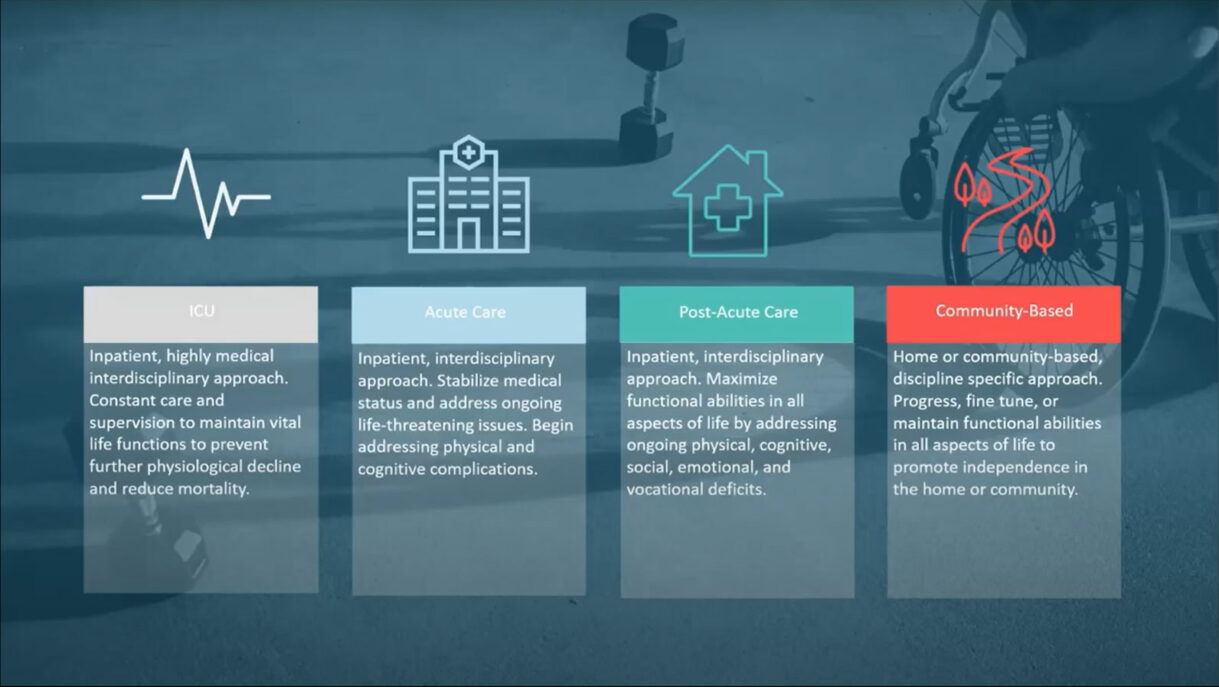
Again, with our folks with brain injuries, spinal cord injuries, chronic pain to a degree, limb loss for sure, typically we see the first two levels of the continuum: ICU and acute care. Those are pretty standard. But you can see the next two, post-acute care and community-based, is really where there’s a little bit of a fork in the road.
ICU
Just to start, ICU really is meant for a really highly medical and interdisciplinary approach. These are really very close to injury. So at this level of the continuum, we’re really trying to maintain vital functions. They are in a hospital setting and oftentimes very unstable, and we need to make sure that there’s no further decline. Hopefully, essentially we’re keeping people alive here and setting them up for the next levels.
Acute Care
Then you move on to the acute care level. In a lot of ways, it’s similar in the sense that the medical focus is front and center, but you still have this interdisciplinary approach. As they stabilize medically, we can start moving past addressing life-threatening issues, and we can begin to… in the cases where there’s cognitive issues, physical issues, other complications that might be available, that’s something that ends up being a big piece of this.
Post-Acute Care
Then we get down to really… as we go through our modules, we’re going to focus mostly on this post-acute level and the community-based level. The inpatient side of things is still a pretty common thing at the post-acute level of care. If you’re at this level, hopefully you have a pretty interdisciplinary approach. Here at QLI, our post-acute program, we have all the disciplines, PT/OT, speech, psychology, nursing, and a whole host of other things that help people get back to life. But really what we’re able to do is because these folks are medically stable, that ends up being even lesser of a focus. Then we’re really ramping up on the physical and the cognitive, emotional and vocational aspects of things. So I don’t know if, Brad, you want to talk a little bit more about this part of it.
Brad Dexter PT, DPT [03:16]:
I’m hearing kind of an increase in intensity along the way. If someone becomes a little bit more medically stable, we’re able to increase the intensity at which they’re able to work, too. So post-acute care side of things, it really takes a large team of people to be pushing that person forward, and, like we often say at QLI, picking up the pieces of life, again, putting those pieces together because it’s complex. It’s not just the physical aspect or the cognitive aspect or the medical aspect. All of those things are going to run together, and it takes a big group of people to interact well and communicate well to piece that back together.
Steve Kerschke, PT [03:55]:
Still highly supported.
Community-Based Care
Then as we look at the community-based level of care, as it suggests, these folks are back at home. It could maybe be in assisted living, but they’re really out interacting with the real world at this point in time. Some individuals, depending on what their care has looked like up to this point, they still have a lot of aspects of their life to work on. It could be supported by caregivers or family members, their support system to whatever degree, but hopefully they’ve moved into this continuum in a relatively independent nature. Maybe they’re going back to work, volunteer jobs, school, whatever it might be, or maybe they’re just simply trying to get through their day around the house and reintegrate into parenting and being a spouse and that sort of thing.
Brad Dexter PT, DPT [04:44]:
Yep, absolutely. That’s what I was thinking about. It’s like not just the work or a community-based, but even just in the home. What are they able to do? How do they return back into some of those same roles?
Steve Kerschke, PT [04:54]:
It’s all set up by that post-acute level of care and in some cases the acute level, but hopefully we’re envisioning what home looks like. Depending on deficits, whether it’d be cognitive or physical, that really dictates what they’re going to be able to do once they get here. Brad, you also mentioned this full continuum, and we’ll get to the next slide here, too, in terms of intensity, medical intensity and therapeutic intensity.
The Continuum of Care in Terms of Time
But before we do that, this really is a more visual take on what the continuum looks like in terms of time. So often time we see ICU, assuming there’s no big complications and they move through that, many of the clients that we work with are going to spend a relatively short period of time in ICU comparatively. They’ll get to acute care a little bit longer. Post-acute care, if they happen to go, we tend to see people up to 80 days or so on average. It could be longer. It could be shorter. Then you see the community-based level of care is quite a bit longer, hopefully indefinitely. There’s some considerations there, too. But if all goes as planned, this is a pretty standard continuum.
Brad Dexter PT, DPT [06:08]:
We kind of hit on that intensity piece earlier. As the medical intensity is decreasing, like I said, the therapeutic intensity can really go up. It seems like common sense. If someone is just having their life saved, they’re going through a lot of procedures or even just trying to become a little bit more alert after a catastrophic type of injury, there’s not going to be a whole lot that you can do. You’re kind of in life saving mode. But as a person becomes a little bit more aware as injuries, orthopedic injuries, muscle injuries heal and become a little bit more stable, well, now we can start to work with them a little bit more. Even between the acute rehab setting and the post-acute rehab setting, there can be a significant increase in the level of intensity purely because of the amount of time that’s gone by and the healing that’s allowed to happen.
Steve Kerschke, PT [07:06]:
Some of this is just precautionary, so they might be non-weight bearing or have some other considerations that essentially make it so you can’t increase the intensity, or they just may not be in a spot where they can participate enough or even the fatigue, whether it’d be physical or cognitive, is very limiting in that regard. The other thing I think that we see is it’s not only physical in nature. So as they become more medically stable, certainly the physical component is a consideration, but we can start to focus on the cognitive aspects of life, the emotional and social aspects of life. So we start to look at, okay, what are they going to have to do in the real world? Let’s start to introduce those to therapy, and that in and of itself adds to the complexity.
Brad Dexter PT, DPT [07:51]:
I even think back to some of the learning principles that we talked about in Module 1 and the fact that if we push someone too far outside of their comfort zone, which in this case I think about too much intensity, too fast, that could push them over the edge to failure, too.
Steve Kerschke, PT [08:07]:
So we’re talking about timing. We’re talking about, hopefully, that medical component starts to subside, and then really we can ramp up. But there’s a lot of decision making that happens in between there. Definitely in terms of how we look at things, having a certain level of expertise and understanding when to push, when not to, I think is really, really important.
Brad Dexter PT, DPT [08:27]:
Absolutely.
Outcome Predictability and the Continuum of Care
Steve Kerschke, PT [08:28]:
I think this also leads to this next slide where we talk about predictability. Right at the very beginning, it’s pretty volatile in nature. We might even be wondering if the person’s going to live, unfortunately, at the ICU level. If they do live, predicting what’s going to happen in the future at this point in the continuum is really, really hard. But as you move through, especially into the post-acute level and even the community-based level, things hopefully are becoming more stable. Then, again, for someone who’s worked with this population quite a bit, we should be able to make a pretty good prediction as to their level of care. How much support are they going to need? Are they going to be able to get back to work, or what are they going to do with their day? Not that progress stops here, but it, again, becomes more predictable. I don’t know. Maybe you talk a little bit about your decision making once it gets down to it.
Brad Dexter PT, DPT [09:21]:
Oftentimes, you’re looking at trend lines. How far post-injury is that person? What does their rate of progress look like? Again, like you said, that could change. It doesn’t mean that it’s always going to be like that. If someone hasn’t made a lot of progress, it doesn’t mean that they won’t take off at some point after a catastrophic injury. But if they’re trending in a good direction over the last three months, well, that helps me as a clinician then start to say, “Gosh, given what they’ve been doing and the type of injury that they have, here’s how I might start making decisions about durable medical equipment or the amount of help that that person or support that person is going to need in the long run or their potential to return to work or driving or whatever that may be.
Steve Kerschke, PT [10:04]:
Maybe let’s talk a little bit more about what we’ve seen on the good side and the bad side of this. So let’s maybe look at, if you happen to be at the ICU or acute care level and you have family members who definitely want to understand, “What should we expect here?” what’s your approach there? How do you navigate that? How does that maybe compare to, I’ll say, luxury that you have at the post-acute and maybe the community-based level. How does that differ? As a clinician, how do you navigate that?
Brad Dexter PT, DPT [10:34]:
I haven’t ever worked in the ICU level of care, but I’m thinking something that I’ve heard from a number of people over the years is that they get told this definitive answer early on in that process, and that’s what sticks in their mind. It either creates a lot of hope, or it makes people really mad. They want answers up front. So I think physicians can be put in really difficult positions when they’re asked, “Hey, what is my loved one’s life going to look like? What should we be expecting? I would caution people to give a definitive answer at that moment because we’ve seen so many people that completely beat the odds, or they’ve been told something, “Your loved one will never walk again. They won’t have a level of communication like they ever did prior to or cognitive functioning,” but they completely, again, defy the odds and look totally different six months, nine months, 12 months down the line.
Steve Kerschke, PT [11:33]:
Well, and I think really what you’re getting at is, how do you provide this level of hope and optimism but then balance that with being realistic?
Brad Dexter PT, DPT [11:40]:
Realistic, yeah.
Steve Kerschke, PT [11:42]:
I do think that there’s this certain pressure to make sure that you set people up and help them understand, “Here’s the worst-case scenario.” That would be a really hard position. We’ve been in that position. We just happen to be later in the game. But no one ever wants to be the person that crushes hopes and dreams, nor do I think we are in the position to do that. I think you and I both take the approach of, “Look, we don’t have a crystal ball. We’ve seen a lot of folks in your positions. Typically, here’s what happens. But we’re going to do this, this, and this, and hopefully we can make some progress.”
One more thing. Let’s get back to your decision making about, let’s just say DME, so durable medical equipment. I think of this especially in terms of wheelchair choices. We get that individual, maybe a spinal cord injury, who might benefit from a power wheelchair as well as a manual wheelchair. You and I have seen plenty of times where they outgrow maybe that power wheelchair and no longer need it, or they outgrow both of them if they happen to be incomplete in nature and they’re up walking around. Talk about how we make those decisions and the value of waiting a little bit further into the continuum if you have that luxury to do so.
Brad Dexter PT, DPT [12:51]:
Again, back to trend lines a little bit. Let’s say that I’ve had a person that has a lower cervical spine, level spinal cord injury, but I know that it’s an incomplete injury. Maybe they started out as maybe 50% incomplete, what we would call an ASIA B to ASIA C type of spinal cord injury, but they’ve progressed over the last three to six months maybe before they get to us at QLI to a level that’s even more incomplete. Functionally they’ve been able to go from just maybe standing with help to starting to take steps or even taking steps without help, too. I start to think, “Well, how far could this person go? Are they at just a home-based level of walking? Is it a community-based level of walking? Will they need some kind of a power wheelchair or power mobility device to get them around in the community and help them access that or not?
I think if you’re in a position where you’re having to make those decisions three months after an injury, oftentimes we get lots of people put in that position where they’re expected to identify the equipment needed for that individual over the long haul. Someone may come to us with a power wheelchair and leave, and they don’t even need a wheelchair anymore because they’re up, and they’re walking, and they’re on their feet. It is a case that we have more incomplete spinal cord injuries now than we ever have because of those advances in medicine and advances in response time to those spinal cord injuries, too. So it does make that decision-making process a little bit more difficult. But in order for someone to need that chair long term, they’re going to have to have some level of an need especially in a community setting over longer walking distances because oftentimes I want people to spend as much time on their feet as possible as long as they’re safe.
Steve Kerschke, PT [14:47]:
Well, and I think that’s the whole point of this. If we understand what the continuum holds in the future and hopefully we make better decisions early on with the best information that we have knowing that we don’t have everything that we wish we would have, we don’t understand exactly what’s going to happen, and we’re going to make some mistakes along the way. Hopefully, we keep learning from that.
Levels of Support in the Continuum of Care
The level of support contributes to this as well. So just as the volatility and predictability is extremely low, they’re in situations where the support is really, really high. So they’re in a hospital setting. They’re with physicians. There’s nurses right down the hall. If there’s a medical emergency, there’s quite a bit of support with that. As a result, people’s abilities can be masked, or what they might look like in a really structured formal setting may not be predictive of what they’re going to look like in the real world. So the nice thing about moving through the continuum is that the support hopefully decreases. We can start doing things out in the community outside of a really formal hospital-based setting, and we get a really clear look at what someone can look like. So let’s talk a little bit more about what does that look like at the post-acute level and maybe what does that look like at the community-based level and how are they the same or different.
Brad Dexter PT, DPT [16:10]:
Just thinking about the level of support needed at post-acute care level, we touched on this earlier. At QLI, we have PT/OT, speech, nursing, psychology, some physician support, life care, life skills, life path services. So there’s a number of people that are touch points there, and, again, trying to piece the person’s life back together, give them a vision, and help them get some ownership and autonomy over life again because people have had a lot of control stripped away from them. Then the ultimate goal is that when we get to that community level of care, it’s you driving a lot of that as the individual with maybe your close support system. Maybe that’s a spouse or friends or significant other that is involved with you, children, and then your medical support team that’s there, but is more fragmented and not seeing you on a daily basis.
Steve Kerschke, PT [17:07]:
Well, and I think it’s a constraint in and of itself. Because there’s this level of support, and as providers, we work really hard to start to scale it back so that we can get a really clear picture of what this person’s going to be able to do and so that person in their network can get an idea of what’s going to be needed when they get home. But if we don’t do a good job of, call it, simulating, but even simulating is not really all that realistic because we can’t simulate spontaneity. We can’t simulate random things that happen in our [inaudible 00:17:39].
Brad Dexter PT, DPT [17:39]:
Novel tasks.
Steve Kerschke, PT [17:40]:
We can’t simulate that. Because we can’t simulate that, there’s going to be a gap even if we do a really good job of that. So I think that’s a really big piece of this is that we want to decrease the support appropriately. We want to integrate the challenges that are going to be faced once we get to the community-based level of care, but we have to be prepared that we’re not going to get quite there. There’s still going to be a percentage that we’re going to have to see and we’re going to have to respond to.
What Does the Therapy Team Look Like?
We talk quite a bit about what a therapy team looks like from ICU really through a post-acute program. It’s pretty extensive. We’ve already mentioned that the support is really, really high. Typically, these individuals are all at the same setting. Obviously the injured person, we have injured worker here. We deal a lot with work comp. The support system is going to be available, any sort of care coordination if that happens to be available and then all of the medical professionals that are involved here.
There’s a couple different ways to look at this. But with the types of injuries that we deal with, we recommend a center of excellence of some sort. Typically, there are centers of excellence at every level in the continuum. It gets a little bit harder to find it as you get further down the road, but we highly recommend that given the level of expertise that it takes to navigate these types of situations. You’re going to find, for the most part, each of these disciplines at those centers of excellence.
But once you get past the post-acute level, an interdisciplinary therapy team is oftentimes a bit hard to find. We’ve pictured the ideal scenario. This isn’t always the case. Hopefully, the injured person and their support system are really closely tied to each other. They might be in the same city, or they at least have a good working relationship, and they have supports in the fashion that they need in order to be successful. Granted, this isn’t always the case, and it looks very different from person to person, but this is the ideal. Then they’re going to have some physician support on board. The specialties of those physicians is going to vary depending on their cognitive or physical abilities or whatever else they have going on.
Then we’ve just outlined PT/OT, speech, and psychology here. It could be nutrition. This certainly isn’t meant to be all-inclusive either. But if you can get those PT/OT, speech, psychology-like disciplines all in one setting or all with a team that’s working really closely together, we believe that the outcome is the best in that scenario because there’s a high level of collaboration and communication that needs to happen. You work on a therapy team. Talk a little bit more about what that looks like for you.
Brad Dexter PT, DPT [20:31]:
I guess in my 11 years of being a physical therapist, one of the things that I’ve appreciated the most, both working at QLI and also in continued tele-rehab, the fact that I’m not on an island. As a provider, I get viewpoints and I get perspectives from my occupational therapist, the psychologist working with the individual, speech therapist, and having a few more heads at the table always, I think, leads to some better outcomes. There are cases where it’s just one discipline with a person working especially on the tele-rehab side, but I love not working on an island and being able to work together in a team to make sure that we’re looking at things from all different angles.
Steve Kerschke, PT [21:15]:
Well, and it allows you to be really nimble, too. So having regular, call it, team meetings throughout the week, I wouldn’t say is the norm at the community-based level. We see it quite a bit at the post-acute level. You have weekly meetings where we’re planning and things are moving very, very quickly. Thankfully, they slow down a little bit at the community-based. But I do think that having those meetings allows the therapy team to keep everyone informed: “Here’s where we’re going. Here’s how things are progressing, and if there’s challenges or opportunities to push the limits a little bit, we can respond to that very, very quickly.”
Brad Dexter PT, DPT [21:50]:
I even think within our tele-rehab team, there are times where our psychologists will inform you of something that’s going on with the individual that they may not tell me. That’s not breaking patient confidentiality. It’s just like, “Hey, so-and-so mentioned that this is going on with a brace that they have. Would you mind just checking in with them to make sure that that’s okay?” Or me being able to say the occupational therapist, “Hey, this person, it seems like they might be having some issues maybe reintegrating into the community and maybe even vocationally getting back to volunteer opportunities. What do you think about helping them with that?”
Steve Kerschke, PT [22:25]:
I think the other component is from a learning perspective. How many times might they be out in the community and they happen to be with the speech therapist or the occupational therapist and they’re working on mobility and walking and whatever else they might be doing out there? It’s an opportunity to be supported by someone who understands, like, “Oh, I know Brad’s working on this. How can I be supportive of that and add a few repetitions of that along the way?” So we boost the intensity of the program just by having some collaboration along the way.
Brad Dexter PT, DPT [22:57]:
I think my care is made better by having those teammates around me.
Steve Kerschke, PT [23:00]:
Absolutely. So a really unique component, I think, to our program. If you don’t happen to make it to our program, I think it’s just something that you-
Brad Dexter PT, DPT [23:08]:
You should look for.
Steve Kerschke, PT [23:09]:
… should look into. Yeah, for sure.
Conclusion
That wraps up our Module Number 2. Obviously, we have a couple more to go to. Hopefully by the end of this, our listeners can understand here’s the different levels of the continuum. Here’s what’s important at each level. Here’s a few things I should be looking for. Hopefully, the other two modules we have coming will support this one. Thanks again for joining me today and always fun to not have to present on my own.
Interdisciplinary Approach A catastrophic injury, like a traumatic brain or spinal cord injury is a life-altering event that impacts an individual’s physical, cognitive, and emotional abilities. The road to recovery […]
Cross the Bridges We’ve introduced the idea of “Cross the Bridges” in the past. It is a useful metaphor to help injured workers and their support teams visualize, understand, and […]
The Road Trip No one dreams of or prepares for a catastrophic injury, yet at every turn, injured workers and their families are faced with seemingly insurmountable challenges that even […]